The course provided instruction in advanced nursing roles and functions applied to health promotion, health maintenance, health restoration, habilitation, and rehabilitation of infants, children, and adolescents with existing or potential health problems; critical thinking used to assess, diagnose, intervene, and promote continuity of care with clients of these ages irrespective of setting. My clinical experience was at the Children’s Center in Greenwood, SC.
Total Patients: 270
28 URI
46 well visits (immunizations, screenings)
7 asthma
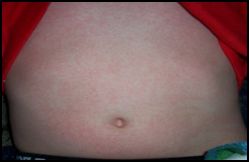
2 roseola
7 otitis media
8 influenza
5 strep throat
2 sinusitis
1 pneumonia
2 constipation
5 ADHD
1 erythema toxicans
1 UTI
1 nephrosis
1 cat scratch fever
1 scabies
3 croup
1 mono
2 allergic rhinitis
3 GERD
2 umbilical hernia
2 sexual abuse
2 suture removal
1 tinea versicolor
1 erythema multiforme
1 shingles
2 sleep apnea
4 tinea capitis
15 pre-school physicals
9 rashes
Preceptor:
Cheryl Platt, PNP
Child & Adolescent Daily Patient Logs:
Preceptor Evaluation:
Course Project:
Protocol for Roseola
Definition: Acute viral infection caused by the human herpesvirus -6 (HHV-6) that primarily occurs in children under 3 years of age. Pathogenesis: Children become infected by asymptomatic shedding of the virus in oral, nasal, or conjunctival secretions. Incubation period ranges from 5-15 days. Children are contagious during the febrile phase before the appearance of the exanthem (rash).
Symptomatic Presentation:
Acute onset of prodromal fever lasting 3-7 days. Fever usually between 101˚F (83.3˚C) – 103˚F (39.5˚C). Fever of 106˚F (41˚C) may cause febrile seizures.
Mild adenopathy of the cervical and posterior occipital areas.
Inflamed tympanic membranes without bulging or effusion.
URI symptoms: rhinitis, sore throat with small maculopapular lesions on the soft palate and uvula.
Abrupt resolution of fever and eruption of rash on trunk spreading to face and extremities. The maculopapular rash is discrete, rose-colored pink, 2-3 mm in diameter, fades on pressure, rarely coalesces (fuses) and lasts only one or two days.
Assess for lethargy (possible encephalitis) and respiratory distress.
Inspect skin for rash. See table for comparison of skin eruptions similar to roseola.
Note other symptoms such as coryza, cough, patches on throat, watery eyes to rule out other viral conditions. Maculopapular lesions present on soft palate & uvula with roseola.
Assess neck for nuchal rigidity (possible meningitis) and adenopathy. Adenopathy present with roseola.
Auscultate heart and lungs. Normal findings are present with roseola.
No diagnostic tests needed unless diagnosis is uncertain. May consider serology test to document rise in antibody titer for HHV-6 (Burns, 511).
Supportive Treatments:
Encourage fluids to prevent dehydration from high fever.
Acetaminophen 10-15mg/kg PO/PR q 4-6h prn for fever >101˚F. Not to exceed 4 grams (4,000mg)/24h.
Patient Education:
Reassure parents that the high fever does not mean a serious disease. Fevers lasting more than 7 days need to return for follow-up treatment.
Return for further evaluation if child is lethargic, poor fluid intake, cough, and is irritable. These symptoms suggest another disease process other than roseola.
COMPARISON OF OTHER RASHES TO ROSEOLA
Roseola: Discrete, rose-colored maculopapular rash, 2-3mm, begins on trunk and spreads to face and extremities, follows acute fever.
Scarlet Fever: Diffuse, red sandpaper-like eruptions measuring 1-2 mm. Follows infection of Group A beta-hemolytic streptococcus.
Pityriasis Rosea-Like Rash: Generalized discrete and confluent round to oval 1-3 mm., red with annular papules and plaques. Typical of drug reaction.
Rubella/German Measles: Pink, maculopapular eruption which begins on the face and spreads to trunk and extremities.
Rubeola/Measles: Diffuse red popular eruptions with confluence on face that spread over 3 days to the trunk and extremities. Serologic studies are positive for measles. Koplik’s spots.
Burns, C., Dunn, A., Brady, M., Barber, N., & Blosser, C. (2009). Pediatric primary care (4th ed.). St. Louis:
Saunders Elsevier, 510-511.
Epocrites.com/Tylenol Uphold, C., & Graham, M. (2003). Clinical guidelines in family practice (4th ed.). Gainesville, FL: Barmarrae Book, Inc., 238-239.